
ECG Course (PDT) Details:
ECG Course (PDT). Mobile No: 01797-522136,01987-073965.Hotline:01969947171. ECG Courses (PDT) are ECG Course (PDT) 6 Months, ECG Course (PDT) 1 Year, ECG Course (PDT) 2 Years. 6 Months Course Fee 35,500/-, 1 Years Course Fee 70,500/-, 2 Years Course Fee 1,30,500/-.
Location of ECG Course (PDT)
ECG Course (PDT) . Mobile Number.01987073965.01797522136,HotLine-01969947171 HRTD Medical Institute , Abdul Ali Madbor Mention, Section-6, Block-Kha, Road-1, Plot-11, Mirpur-10 (Gol-Chattar) Metro Rail Pilar NO-249, Dhaka-1216. It is situated by the West Side of Agrani Bank, the South Side of Fire Service, Islami Bank, Janata Bank, Social Islami Bank, Medinova, Ibrahim Diabetic Hospital, the North Side of Baitul Mamur Jame Mosjid, Grave of Baitul Mamur Jame Mosjid, and East Side of Maliha Apartment.
Course Fee for ECG Course (PDT) 6 Months
Course Fee for ECG Course (PDT) 6 Months at HRTD Medical Institute. Admission Fee=15,500/-,Monthly Fee 3000×6=18,000/-,Exam Fee=2000, Total Course Fee=35,500/-.This Course Contains 4 Subjects .Exam Mark 400.
Course Fee for ECG Course (PDT) 1 Year
Course Fee for ECG Course (PDT) 1 Year at HRTD Medical Institute. Admission Fee=20,500/-,Monthly Fee 3500×12=42,000/-,Exam Fee=4000×2=8000, Total Course Fee=70,500/-.This Course Contains 8 Subjects .Exam Mark 800.
Course Fee for ECG Course (PDT) 2 Years
Course Fee for ECG Course (PDT) 2 Years at HRTD Medical Institute. Admission Fee=30,500/-,Monthly Fee 3500 x 24=84,000/-,Exam Fee=4000×4=16,000, Total Course. Fee=1,30,500/-.This Course Contains 16 Subjects .Exam Mark 1600.
Subjects for ECG Course (PDT) 6 Months
This 6 Months Course contains 4 subjects. Mobile No: 01987073965.01797522136,HotLine-01969947171.
- Cardiovascular Anatomy & Physiology
- Cardio Conductive System & Coronary Blood Circulation
- Fundamentals of Electro Cardiography
- Practicals-1 (ECG Led Placement & Machine Operator) & Graph Analysis
Subjects for ECG Course (PDT) 1 Year
This 1 Year Course contains 8 subjects. Mobile No: 01987073965.01797522136,HotLine-01969947171
1st Semester
- Cardiovascular Anatomy & Physiology
- Cardio Conductive System & Coronary Blood Circulation-1
- Fundamentals of Electro Cardiography
- Practicals-1 (ECG Led Placement & Machine Operators)
2nd Semester
- Cardio Conductive System & Coronary Blood Circulation-2 & 3
- ECG Interpretation and Analysisis
- Patient Management for ECG
- Practical-2 & Graph Analysis
Some Subjects Details for ECG Course (PDT) Given Below
Cardiovascular Anatomy & Physiology for ECG Course (PDT)
Definition (সংজ্ঞা)
Cardiovascular Anatomy & Physiology হলো এমন একটি বিষয় যেখানে হৃদ্যন্ত্র (Heart), রক্ত (Blood) ও রক্তনালী (Blood vessels) এর গঠন (Structure) এবং কার্যপ্রণালী (Function) বিস্তারিতভাবে অধ্যয়ন করা হয়।
The cardiovascular system consists of the heart, blood vessels (arteries, veins, capillaries), and blood, designed to deliver oxygen/nutrients and remove waste. The heart, a four-chambered muscular pump, uses alternating contraction (systole) and relaxation (diastole) to circulate blood through the pulmonary (lungs) and systemic (body) circuits, maintaining a normal heart rate (sinus rhythm).
Cardiovascular Anatomy
- Heart Location and Structure: Located in the thoracic mediastinum, the heart weighs 250-350g and is enclosed in the pericardium, a protective sac. The heart wall has three layers: epicardium (outer), myocardium (muscular middle), and endocardium (inner).
- Heart Chambers: The heart has four chambers: right/left atria (receiving) and right/left ventricles (pumping).
- Heart Valves: Ensure one-way flow:
- Atrioventricular (AV) Valves: Tricuspid (right) and Mitral/Bicuspid (left).
- Semilunar Valves: Pulmonic (right) and Aortic (left).
- Blood Vessels:
- Arteries: Carry blood away from the heart (thick, muscular).
- Veins: Return blood to the heart (contain valves).
- Capillaries: Tiny vessels for nutrient/gas exchange.
- Coronary Circulation: Supplies oxygenated blood directly to the heart muscle via the right and left coronary arteries
Chambers of Heart
| Chamber | Function |
|---|---|
| Right Atrium | Body থেকে blood নেয় |
| Right Ventricle | Lungs-এ পাঠায় |
| Left Atrium | Lungs থেকে blood নেয় |
| Left Ventricle | Body-তে পাঠায় |
Valves
| Valve | Function |
|---|---|
| Tricuspid | Backflow আটকায় |
| Mitral | Backflow আটকায় |
| Pulmonary | RV → Lungs |
| Aortic | LV → Body |
Cardiovascular Physiology
- Blood Flow Circuit: Deoxygenated blood returns from the body via superior/inferior vena cavae
right atrium
tricuspid valve
right ventricle
pulmonic valve
pulmonary arteries
lungs (oxygenation)
pulmonary veins
left atrium
mitral valve
left ventricle
aortic valve
aorta
body.
- Cardiac Cycle:
- Systole (Contraction): Ventricles contract, closing AV valves and pumping blood into arteries.
- Diastole (Relaxation): Ventricles relax, closing semilunar valves and filling with blood from atria.
- Electrical Conduction System: Initiates and spreads the heartbeat:
- Sinoatrial (SA) node: Natural pacemaker in the right atrium.
- Atrioventricular (AV) node: Delays signal for ventricular filling.
- Bundle of His/Purkinje fibers: Transmit impulses throughout ventricles.
- Cardiac Output: The amount of blood pumped per minute, calculated as
.
- Regulation: The autonomic nervous system adjusts heart rate and contractility based on metabolic demand
Cardio Conductive System & Coronary Blood Circulation
Cardio Conductive System
Cardio Conductive System হলো হৃদ্যন্ত্রের এমন একটি ইলেকট্রিক্যাল সিস্টেম
যা নিজে নিজে impulse তৈরি করে এবং ছড়িয়ে দিয়ে heart beat নিয়ন্ত্রণ করে।
The cardiac conduction system (CCS) is a specialized network of nodes and muscle fibers that coordinate the heart’s rhythmic contractions. Unlike standard muscle cells, these “conducting cells” primarily carry electrical signals, ensuring the atria and ventricles squeeze in a precise, timed sequence.
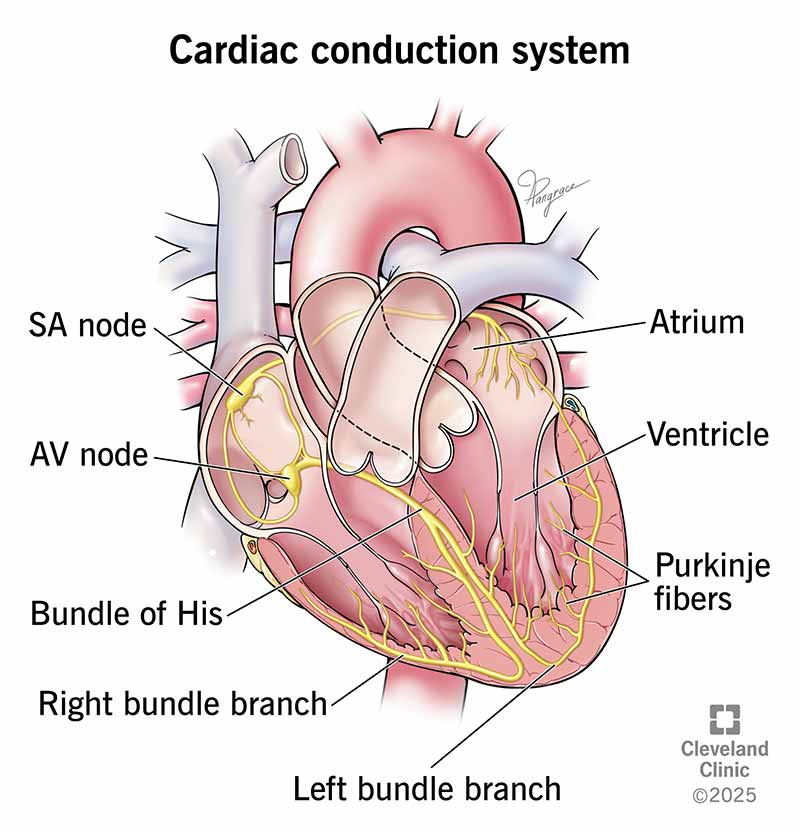
The Electrical Pathway
Each heartbeat follows a specific route through the heart’s “wiring”
- Sinoatrial (SA) Node: Located in the upper right atrium, it is the heart’s natural pacemaker. It spontaneously generates the initial electrical impulse (60–100 times per minute) that triggers the heartbeat.
- Atrial Conduction: The signal spreads across both atria, causing them to contract and push blood into the ventricles. This activity is visible as the P wave on an ECG.
- Atrioventricular (AV) Node: Situated between the atria and ventricles, this node acts as a gatekeeper. It briefly delays the signal (approx. 120ms) to ensure the atria have completely emptied their blood before the ventricles contract.
- Bundle of His: After the delay, the impulse travels through this bundle of fibers located in the interventricular septum. It is the only electrical bridge between the atria and the ventricles.
- Bundle Branches: The Bundle of His splits into left and right branches, which carry the signal toward the apex (bottom) of each respective ventricle.
- Purkinje Fibers: These fine fibers spread rapidly through the ventricular walls. They trigger a synchronized, powerful contraction of the ventricles, pumping blood to the lungs and the rest of the body. This creates the QRS complex on an ECG.
Backup Systems (Automaticity)
If the primary pacemaker fails, other parts of the system can take over at slower rates:
- AV Node: Can pace the heart at 40–60 beats per minute.
- His-Purkinje System: Can provide a “last resort” rhythm of 20–40 beats per minute
Clinical Relevance
- Heart Block: Impaired signals between atria and ventricles, often requiring an artificial pacemaker.
- Bundle Branch Block: A delay in one of the bundle branches, which can cause the ventricles to beat out of sync.
Coronary Blood Circulation
Coronary circulation is the dedicated system that delivers oxygen-rich blood to the heart muscle (myocardium) and removes deoxygenated waste. Because the heart is a highly active muscle that never rests, it requires a continuous supply of nutrients, accounting for approximately 5% of total cardiac output.
1. Arterial Supply (The “Crown”)
The coronary arteries originate from the aortic root, specifically from the left and right aortic sinuses just above the aortic valve.
- Left Main Coronary Artery (LMCA): Often called the “widow-maker” due to its critical role, it divides into:
- Left Anterior Descending (LAD): Supplies the front of the left ventricle and the anterior two-thirds of the interventricular septum.
- Circumflex Artery (LCx): Circles the heart to supply the left atrium and the side and back of the left ventricle.
- Right Coronary Artery (RCA): Supplies the right atrium and ventricle, the SA and AV nodes (in most people), and the bottom of the left ventricle.
- Posterior Descending Artery (PDA): In 70–85% of people (right-dominant), this branch arises from the RCA to supply the back of the heart
2. Venous Drainage
Once oxygen is used, deoxygenated blood is collected by cardiac veins and returned to the right atrium
Fundamentals of Electro Cardiography for ECG Course
An Electrocardiogram (ECG or EKG) measures the heart’s electrical activity over time, using electrodes on the skin to generate a graph of waves (P, QRS, T) and intervals that represent heart chamber depolarization (contraction) and repolarization (relaxation). A standard 12-lead ECG helps diagnose arrhythmias, heart attacks, and electrical conduction issues, with normal rates typically between 60–100 beats per minute.
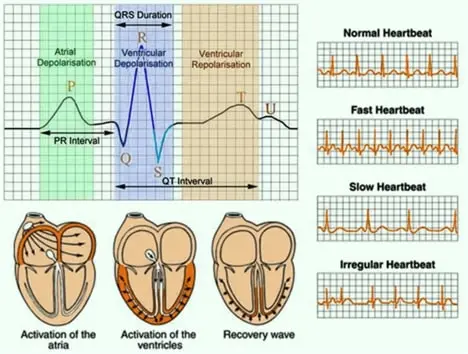
Components of an ECG Complex
- P Wave: Represents atrial contraction (depolarization), marking the start of the heartbeat.
- PR Interval: The time it takes for the electrical signal to travel from the atria to the ventricles (0.12 – 0.20 sec).
- QRS Complex: Represents ventricular depolarization/contraction; it is usually 0.06 – 0.10 seconds in duration.
- ST Segment: Represents the completion of ventricular depolarization and start of repolarization, connecting the QRS to the T wave.
- T Wave: Represents ventricular relaxation (repolarization).
- QT Interval: Total time for ventricular depolarization and repolarization, usually lasting 0.35 – 0.45 seconds
Basic ECG Interpretation Steps
- Rate: Normal rate is 60–100 beats per minute (bpm). Bradycardia is <60 bpm, and Tachycardia is >100 bpm.
- Rhythm: Assess if the R-R intervals are consistent, indicating a regular sinus rhythm.
- P wave: Check if a P wave precedes each QRS complex.
- QRS Width: Ensure the QRS complex is not too wide, which could indicate a block.
ECG Basics Tips
- Small Square: Represents 0.04 seconds and 0.1 mV.
- Large Square: Represents 0.2 seconds and 0.5 mV.
- 300-150-100-75-60-50 Rule: Used to determine heart rate by counting large squares between R-waves
ECG Interpretation and Analysisis for ECG Course
ECG interpretation is a systematic process used to analyze the heart’s electrical activity, involving evaluation of rate, rhythm, axis, and waveform morphology (P-wave, QRS complex, ST-segment, T-wave). A standard 12-lead ECG is crucial for diagnosing arrhythmias, myocardial infarction, and conduction abnormalities, ensuring a proper clinical context is maintained.
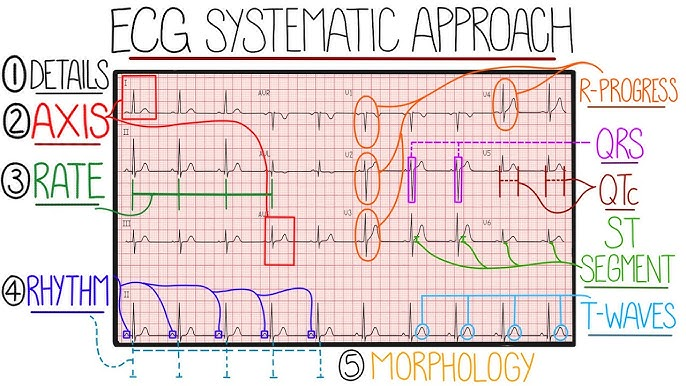
Systematic ECG Interpretation Steps (12-Lead ECG):
- 1. Technical Quality & Calibration: Verify patient details, ensure standard calibration (25 mm/s, 10 mm/mV), and check for artifact.
- 2. Rate: Calculate heart rate (normal 60–100 bpm). For regular rhythms, divide 300 by the number of large squares between R-R intervals.
- 3. Rhythm: Assess R-R intervals for regularity and identify P-wave presence (normal sinus rhythm has P-waves preceding every QRS).
- 4. Axis: Determine the overall direction of electrical spread. Normal axis is
to
(positive QRS in I and II).
- 5. Intervals:
- PR Interval: Normally 120–200 ms (3–5 small squares). Prolongation suggests AV blocks.
- QRS Duration: Normally
ms (
small squares). Wider complexes suggest bundle branch blocks.
- QT Interval: Corrected for heart rate (QTc), normally
ms in men and
ms in women, crucial for assessing risk of torsades de pointes.
- 6. Waves and Segments:
- P-wave: Evaluates atrial depolarization.
- ST-segment: Evaluate for depression or elevation, suggesting ischemia or infarction.
- T-wave: Look for inversions or tenting (hyperkalemia)
Key Normal Values:
- P wave: 2–3 mm high, duration 0.06 – 0.12 sec.
- PR interval: 0.12 – 0.20 sec.
- QRS complex: Duration 0.06 – 0.10 sec.
- Heart rate: 60–100 bpm
Clinical Relevance & Findings:
- Arrhythmias: Examples include Sinus Bradycardia (
bpm), Tachycardia (
bpm), and Atrial Fibrillation.
- Conduction Issues: 1st, 2nd (Mobitz I/II), and 3rd-degree heart blocks.
- Myocardial Infarction: ST elevation (STEMI) or depression indicates acute injury
Patient Management for ECG in ECG Course
ECG patient management involves preparing the patient to ensure accurate, artifact-free tracings by cleaning skin and ensuring a relaxed state. Key steps include explaining the procedure, maintaining privacy, correctly placing 10 electrodes for a 12-lead ECG, and ensuring the patient remains still, quiet, and supine.
Pre-Procedure Management
- Preparation: Advise the patient to avoid lotions, oils, or powders, as these interfere with electrode adhesion.
- Skin Prep: Shave excessive hair and clean skin to ensure good contact.
- Preparation/Restrictions: Ask the patient to remove clothing from the waist up (provide a gown) and remove jewelry.
- Informed Consent: Explain that the test is painless, non-invasive, and lasts only a few minutes.
- Comfort: Ask the patient to lie down, relax, and stay still, as movement or talking can create artifac
Procedure Management
- Electrode Placement: Apply 10 electrodes to the chest and limbs to generate a 12-lead ECG.
- Safety: Ensure the ECG machine is properly grounded.
- Monitoring: If the patient experiences symptoms (e.g., chest pain, dizziness) during the ECG, document them immediately
Post-Procedure Management
- Removal: Remove electrodes and clean adhesive residue from the skin.
- Return to Activity: Patients can immediately return to normal activities.
- Data Management: Verify that the ECG data was correctly recorded and saved to the patient’s electronic health record
Ambulatory ECG Monitoring (Holter/Patch)
- Instructions: Instruct the patient on how to keep a diary of symptoms and activities (e.g., exercise, eating).
- Maintenance: Instruct them not to get the monitor wet (no bathing).
- Troubleshooting: Advise on what to do if an electrode patch falls off
ECG Led Placement & Machine Operators for ECG Course
A standard 12-lead ECG involves the precise placement of 10 electrodes—4 on the limbs and 6 on the chest—to provide 12 different electrical “views” of the heart. Machine operators, often called electrocardiograph technicians or operators, are responsible for patient preparation, ensuring high-quality recordings without interference (artifacts), and maintaining the equipment.
Standard Electrode Placement Locations
Accurate anatomical landmarking is critical to prevent misdiagnosis.
| Electrode | Anatomical Landmark |
|---|---|
| V1 | 4th Intercostal Space (ICS) at the right sternal border. |
| V2 | 4th ICS at the left sternal border. |
| V3 | Midway between V2 and V4. |
| V4 | 5th ICS at the left midclavicular line (imaginary line down from the middle of the collarbone). |
| V5 | Left anterior axillary line, horizontal with V4. |
| V6 | Left mid-axillary line, horizontal with V4 and V5 (directly under the armpit). |
| RA / LA | Right/Left Arm: Fleshy areas of the upper arms or wrists; must be symmetrical. |
| RL / LL | Right/Left Leg: Fleshy areas of the lower legs or ankles; RL acts as the ground. |
Operator Responsibilities & Machine Handling
- Skin Preparation: To reduce electrical resistance, operators must clean the skin with alcohol pads to remove oils and may need to clip excess chest hair.
- Patient Positioning: The patient should ideally be in a supine (flat on back) or semi-Fowler’s position (45° angle). Operators must ensure the patient is relaxed and still to avoid “muscle artifact” (shivering or tension).
- Reducing Artifacts: Operators should ensure electronic devices (like phones) are away from the machine and check that cables are not tangled or over-strained.
- Documentation: Any deviations from standard placement (e.g., due to patient injury or anatomical variation like dextrocardia) must be annotated on the final tracing for the interpreting physician
Common Mnemonics for Color Coding (AHA System)
- Limb Leads: “White on right, snow over grass” (White RA, Green RL); “Smoke over fire” (Black LA, Red LL).
- Precordial Leads: “V1 (Red), V2 (Yellow), V3 (Green), V4 (Brown), V5 (Black), V6 (Purple)”
